
Photo credit: Farrah Skeiky
by Patty Skuster and Heidi Moseson
Medication abortion did not begin with a clinical trial; it began at home as self-managed abortion, or abortion without supervision from a clinician. Decades before the 2000 U.S. Food and Drug Administration’s (FDA) approval of mifepristone for abortion, which is taken alongside misoprostol, feminists in Brazil found an opportunity to self-manage abortion with misoprostol, based on warning labels that cautioned about the risk of miscarriage if taken while pregnant. The genesis of abortion pills was therefore in self-managed abortion with misoprostol alone.
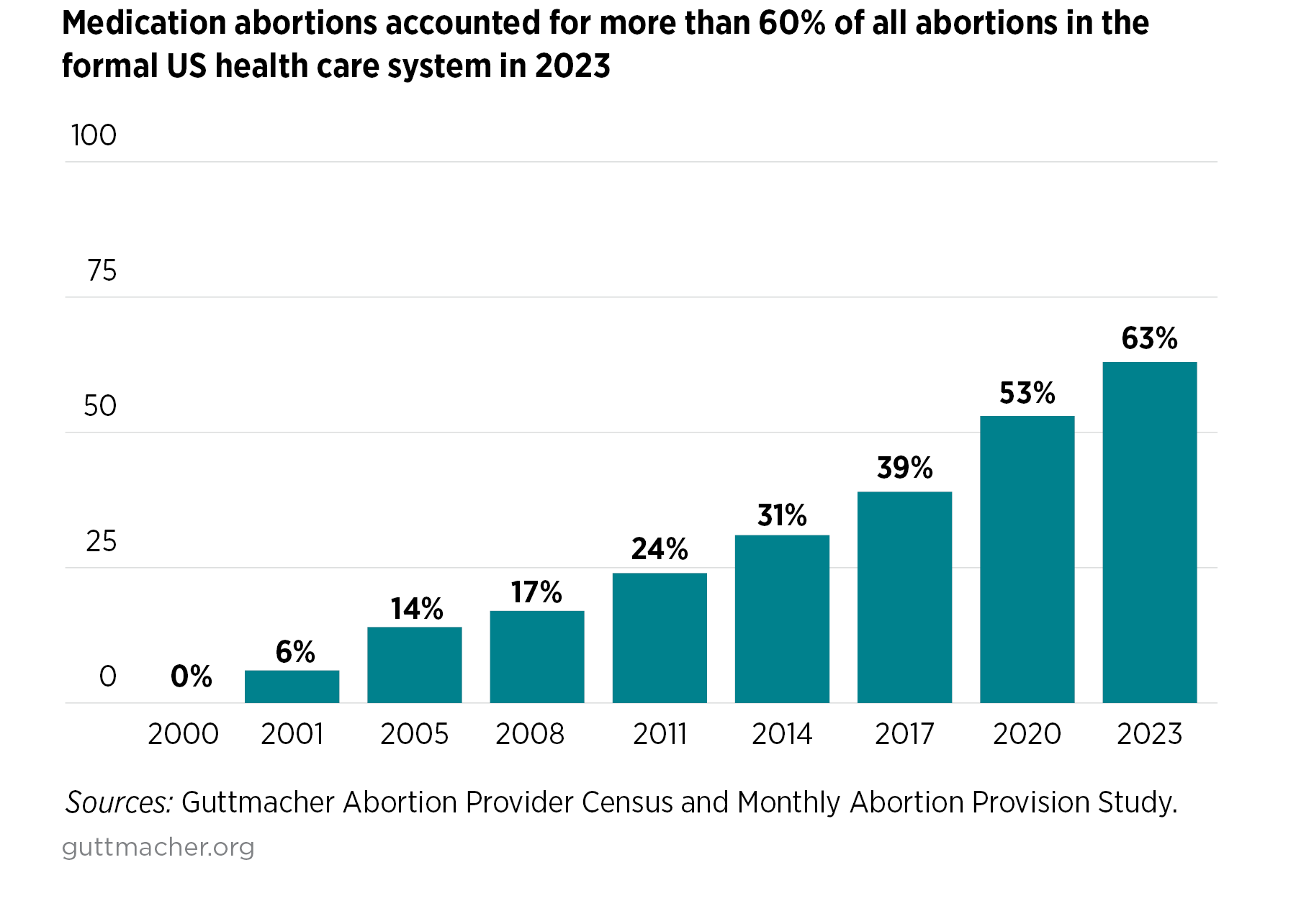
Today, after several decades of clinical trials and heavy regulation of medication abortion, the practice of self-managed abortion with misoprostol-only is once again driving clinical practice. While medication abortion has been increasing in the U.S. since its introduction, major changes in recent years have dramatically increased usage. In 2021, the FDA relaxed enforcement of the requirement for in-person dispensing of mifepristone. This revolutionary change allowed the pills to be sent by mail for the first time, making them much more accessible. When, in 2022, the Supreme Court eviscerated the federal constitutional right to abortion in Dobbs v. Jackson Women’s Health Organization, the resulting abortion clinic closures led to even larger numbers of abortion seekers turning to medication abortion through telehealth and mailed medication from providers in supportive abortion states and clinicians outside the U.S. Combined, medication abortion now accounts for more than half of all abortions in the US.
{kind=link}
Available data show that nearly all medication abortions in the U.S. utilize the combined regimen with mifepristone. Clinical training and protocols encourage use of the combined regimen over the misoprostol-only regimen based on broad interpretations of effectiveness from pooled data on a range of misoprostol-only regimens. Recent, more focused analyses, however, have called for a reevaluation of this tiered approach. Regardless, in abortion-supportive states, misoprostol-only is legal under off-label use, but is rarely offered by U.S.-based clinicians.
Yet, in this new post-Dobbs legal landscape, mifepristone availability has been at risk amid legal attacks on abortion, including a Supreme Court case focused on FDA regulation of mifepristone that was sent back to the lower courts in June 2024. The potential of a second Trump presidency may also increase threats to abortion. Thus, clinicians are reconsidering their options for medication abortion. To determine how to best offer a single drug regimen in the US, they are looking outside the U.S. for lessons from self-managed abortion settings.
Legal attacks on mifepristone availability and abortion overall
To understand passed, pending, and threatened legal challenges to mifepristone’s use, it is instructive to review the history of the medication in the United States. When the FDA initially approved mifepristone in 2000, it did so under a specific regulatory regime typically only applicable to high-risk drugs — despite mifepristone being an extremely safe medication. This was a political decision, not based on scientific evidence. Specifically, the regulatory regime, known as the Risk Evaluation and Mitigation Strategy (REMS) program, imposes onerous requirements for dispensing the drug and has made mifepristone markedly less accessible than any other medication with a similar safety profile. Examples of these requirements have included requiring physicians to observe the patient physically swallow the pill in person, requiring specific training for physicians prescribing the drug, and requiring multiple in-person visits.
But as a result of years of advocacy from the clinical and scientific community, highlighting the disconnect between mifepristone’s excellent safety profile and the burdensome restrictions imposed by the REMS, the FDA has taken steps in more recent years to make the drug more accessible. Among these have included, in 2016, permitting additional cadres of health providers to prescribe the drug and reducing the required in-person visit to one. As mentioned earlier, in 2021, the FDA enabled patients to receive mifepristone by mail by relaxing enforcement of the in-person dispensing requirement. These actions were the subject of the aforementioned unsuccessful challenge at the U.S. Supreme Court. Still, imminently anticipated challenges to the FDA’s authority from different plaintiffs could lead to restrictions on the medication.
Beyond external challenges to the FDA, a future Trump administration could internally use its power to reverse the 2021 FDA decision and enforce the in-person visit requirement, thereby curtailing the mailing of mifepristone. Other FDA action could further restrict access. In addition, a Trump administration could enforce the Comstock Act to curtail not only the mailing of mifepristone but in effect enact a nationwide abortion ban. State lawmakers also have restrictions on abortion pills in their sights; for example, Louisiana enacted a law to classify both mifepristone and misoprostol as controlled substances, which severely limits access to the medications, even for clinical providers.
The promise of misoprostol alone
Whether or not mifepristone is further restricted, another safe and highly effective medication abortion option remains: misoprostol-only, the original medication abortion. In much of the world, abortions with misoprostol alone are the norm. Unlike mifepristone, misoprostol in the U.S. is not subject to a REMS and is generally available at a lower cost in pharmacies and among a wider range of clinicians, particularly those who work with birthing patients. Misoprostol has multiple essential uses beyond treatment for ulcers, including prevention of postpartum hemorrhage, labor induction, miscarriage management, and more.
Recognizing these strengths and considering threatened restrictions on mifepristone, the National Abortion Federation (NAF) and the Society of Family Planning (SFP) put forward a recommended protocol for medication abortion with misoprostol-only as a guide for clinicians who may need to imminently switch away from mifepristone. These guidelines draw on data from around the world, including data on self-managed misoprostol-only abortions. A 2024 synthesis of peer-reviewed research on the NAF- and SFP-endorsed misoprostol-only protocol concluded that this updated regimen is highly safe and effective (with ~82-100% abortions completed), can initiate an abortion process more quickly than the combined regimen from the time of first pill taken, and may be less expensive and more accessible. In clinical trials that have utilized this regimen, 0.5-5.7% of participants have had an ongoing pregnancy at 1-2 weeks following this regimen — which is comparable to the 0.3-5.0% following mifepristone plus misoprostol. Research from self-managed settings suggests that with additional doses of misoprostol and additional time for follow-up, an even greater percentage of people will have a complete abortion without procedural intervention.
The Way Forward
At a moment when access to abortion is constricting in the United States, it is essential to utilize all safe and effective options available, including a misoprostol-only regimen. Clinical providers and all those who support people having abortions should be trained on how to confidently support people through misoprostol-only abortions, including counseling on when to seek care in the event of a failure of any medication abortion regimen.
Just as multiple forms of birth control with differing degrees of effectiveness, cost, accessibility, and timing are offered to people seeking contraceptive care, multiple medication abortion regimens should be offered to people seeking abortion care. People consider many factors when making reproductive decisions and being able to choose the course of care that is best for them is a crucial aspect of high-quality healthcare. Although under-utilized in the U.S., a misoprostol-only regimen is safe and effective, and when offered alongside the combined regimen, may be a powerful strategy for expanding access to abortion overall in the United States.
Patty Skuster is Associate Director of Accreditation and Core MPH teaching faculty at the University of Pennsylvania’s Master’s in Public Health Program, where she teaches courses on global reproductive rights and public health law. Skuster publishes on the effect of abortion law, with interests in self-managed abortion, U.S. foreign policy, and legal risk.
Heidi Moseson (she/her), is a Senior Research Scientist at Ibis Reproductive Health and an epidemiologist by training. Dr. Moseson’s research focuses on evaluating the safety and effectiveness of self-managed medication abortion and measuring the impact of abortion and gender-affirming care restrictions.
Join the discussion
0 people are already talking about this, why not let us know what you think?